
“Exercise is medicine,” states Dr. Jessica Brown. And when she says this, it’s not some catchphrase – but a genuine belief that physical activity needs to be a standard in clinical care. Dr. Brown is so dedicated to this belief that she is changing the face of cancer rehabilitation by using prescriptive exercise to reduce the harmful side effects associated with the disease and its treatments.
For most of Brown’s career, she served as the Clinical Coordinator of the University of Northern Colorado’s Cancer Rehabilitation Institute, where she taught countless courses on cancer rehab. Today, Brown, an Assistant Professor of Exercise Science – Applied Clinical Practice at Carroll University, is perfecting the “Brown’s Phase Program.” Recently, InBodyUSA, a leader in creating body composition technology, asked Brown to present a virtual webinar for their education series. The presentation unquestionably demonstrated how Brown’s Phase Program provides clear and reproducible exercise guidelines and goals for patients who have been diagnosed with cancer.
Endominance was fortunate to meet with Dr. Brown virtually to discuss how the prescriptive exercise program came into existence, why exercise is critical for cancer survivors and those with chronic diseases, and the program’s future in terms of scalability.
How Rehab Centers Are Under-Prescribing Exercise
During Brown’s master’s coursework, she met Dr. Carole M. Schneider, the pioneer of cancer rehab. From that point on – her whole world changed. Brown tells Endominance, “Dr. Schneider had this crazy idea of using exercise prescriptively for cancer patients and that it might be the answer to cancer survivors and the toxicities from chemo and radiation. After being diagnosed with cancer, Schneider started testing it out on herself and some of her friends from treatment, and they found it very effective.” Brown then entered Schneider’s clinic and was “blown away” after seeing how exercise can be altered to help treat cancer patients. After this experience, she had a “light bulb moment” and changed career paths to study clinical exercise physiology and pursue her Ph.D.
During this time, Brown began working with numerous cancer survivors and those with other comorbidities. She recognized that exercise made people feel better during the rehab program and saw an initial improvement. But then she witnessed a plateau. Brown reveals, “I assumed our rehab program was working. The exercise dosage we were giving was correct, and the patients seemed to reach a healthy function level. However, upon further inspection, we noticed the numbers were significantly below baseline and below the dosage of exercise required to continue to achieve benefits across all aspects of health.” Brown discovered rehab centers were under-prescribing exercise.
She also found that many rehab exercise programs do not adequately adhere to the principles of exercise training necessary for safe and effective intervention. They also did not know how much patients could handle and tolerate. With this information in hand, Brown states, “I began researching the dosage of exercise that patients could take based on different treatment types and different points on the cancer continuum with doctors.” This intense research started the journey to phase training.
The Phase Training Study
Brown and her team began a passionate mission: to expand on current cancer rehabilitation protocols and provide a more precise exercise prescription. They fine-tuned the optimal dosage of exercise based on different treatment types and different points on the cancer continuum of care. She states, “I started testing out a completely new model called ‘phase training.’ We were trying to mirror the phases you see in cardiac rehab that insurance is familiar with for reimbursement.” Her team began collecting significant research data, and the results were profound, “We were seeing two to three times the success rate of the previous rehab models,” states Brown.
In terms of specific targets, the study aimed to evaluate the effectiveness of the program on cardiorespiratory fitness (V˙O2peak), muscular strength (MS), and fatigue in cancer survivors during and after treatment. Eighty-one patients completed the entire program with an entry into phase 4, with 71% retention. Other results showed:
- V˙O2peak, leg press MS, chest press MS, and fatigue significantly improved from phase 1 to phase 2 by 13%, 13%, 18%, and −25%, and from phase 2 to phase 3 by 14%, 19%, 26%, and −27%.
- V˙O2peak and chest press MS significantly improved from phase 3 to phase 4 by 4% and 7%, respectively.
The chart below is an overview of the model and breakdown of each phase in the program.
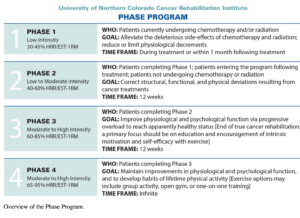
The four-phase system also includes assessments of physiological and psychological variables conducted at the beginning of each phase. Each reassessment marks the completion of the phase and subsequent entry into the next. Entry into the program was determined by patient treatment status. Patients currently undergoing chemotherapy and radiation treatment entered at phase 1, and all posttreatment patients, or those without chemotherapy or radiation treatment, entered at phase 2. Phases 1 through 3 are considered “true cancer rehabilitation.” The program was marked as completed once the patient had entered phase 4.
How Exercise Dosage is Crucial for Success
When asked about the length of each phase, Brown reveals, “The program duration is 12 weeks per phase. We never transition patients out of the program until they achieve phase four, which we consider healthy. When they transition to phase four, we give them community options because this is on them for the rest of their lives. Those with chronic disease start at phase 2, and traditionally, we could progress them into phase 4. However, sometimes we have to do a phase twice or two cycles because we have to help them make substantial lifestyle changes. Without a lifestyle change, they will go back to old habits, and their disease will progress.” The duration of each exercise session was 60 minutes, which included:
- Twenty minutes designated for aerobic exercise.
- Thirty minutes for resistance exercise.
- Ten minutes for flexibility training and balance exercises, incorporating the mind-body connection.
Each mode of aerobic exercise is based on the participants’ assessment results and desired goals in adherence to both the principles of individuality and specificity.
The Future of “Standardized Individualization”
When asked about the future of her phase training program, Brown offers, “My goal is to create several satellite facilities where people can get care through the phase training. However, we see this massive advent of telehealth and virtual training with the pandemic. So we’re creating a telehealth program in perpetuity as another model. So we will have both in-clinic and virtual programs.” In terms of scalability, Brown reveals, “The one-on-one aspect of this program is crucial. Because once you work with the patient and the prescription is made, the next part is walking the patients through the rest of the program. And we need to have people dedicated to creating that part of it. That part of the program is scalable as you can do it one-on-one, as a group, or the patient can do it as homework independently. When a program is reproducible, it’s easier for many people to adopt.”
Brown wants to emphasize that there is no one-size-fits-all for this. She states, “This is where I think this program is vital because it’s standardizing a part that is individualized, which seems paradoxical. How can you standardize individualization? But that’s the trick. Once we solve that problem, it will profoundly impact everyone because everyone is different. You have to find a way to help individuals become healthier in a way that is standardized, reproducible, and trackable.” She also adds, “I want to get this program out there so that every cancer survivor, and those with chronic disease, get the rehab that they need. Everyone has to have access, and insurance has to reimburse some or all of this like they do other specialties and like they do with cardiac rehab.”
Currently, Dr. Brown’s Phase Program is being implemented in clinics and hospitals worldwide and offers clinicians and patients a standardized model to follow. Brown and her team also investigate the positive effects exercise interventions and rehabilitation have on patients diagnosed with chronic diseases and various comorbidities.
